|
|
|
|
|
| |
Quality general dental care with an emphasis on natural esthetics, form and function. Experience with complex restorative, prosthetic and implant treatment.
----------------------------------------------------------------------------------------
INFERIOR ALVEOLAR REPOSITIONING:
CREATING BONE FOR IMPLANT PLACEMENT
When insufficient bone is available in the posterior mandible (lower jaw) above the inferior alveolar nerve the nerve may be repositioned to provide sufficient height for implant placement.
THE ANATOMY OF THE MANDIBLE:
The inferior alveolar nerve enters the lower jaw in the area where the tonsils are normally located and progress through the jaw to exit in the area of the corner of the mouth. (see figure below)
As bone resorbs (shrinks) the amount of bone above the nerve decreases. The position of the nerve does not change in relation to the position in the bone, but as shrinkage occurs the nerve appears to move closer to the surface where the teeth were located. When severe resorption has occurred the nerve may actually be laying on top of the bone just below the gum tissue. This can make wearing a conventional denture extremely difficult due to pain from pressure of the denture on the nerve.
Cross section of the mandible showing the inferior alveolar nerve (red) in relation to a tooth with no bone resorption.
When the tooth is lost, the bone shrinks leaving less available bone for implant placement within the bone

The resulting resorbed ridge.
Visualization of an implant (green) in relation to the nerve (red) in a resorbed mandible.
In a severely resorbed mandible, the nerve (red) may actually be just below the gum tissue and above the bone.
TREATMENT OPTIONS WHEN INSUFFICIENT BONE IS AVAILABLE IN THE POSTERIOR MANDIBLE:
- Inferior alveolar nerve repositioning to permit endosseous implant placement due to insufficient bone height
- Block graft to permit endosseous implant placement due to insufficient bone width
- Placement of plate form implant when insufficient width but sufficient height is present
- Utilization of a subperiosteal implant (subperiosteal implants)
- Utilization of a ramus frame impant (ramus frame implants)
INFERIOR ALVEOLAR NERVE REPOSITIONING PROCEDURE:
Two techniques have been used to move the nerve away from the trajectory of the implants and permit the full height of bone to be used.
The first technique involves removal of the bone overlaying the side of the nerve. The nerve is then carefully removed through the window and the implants are placed. The nerve is then laid back in the channel and the area closed and allowed to heal.
In the second technique, the bone over laying the nerve is removed and a new canal is created below the old canal and the nerve is then moved to its new location. Implants are then placed. The draw back to this technique, if less than 12mm of bone is present between the crest (top of the jaw ridge) and the bottom of the jaw then there may not be sufficient bone to move the nerve to a new canal.
Patients who have either technique may expect some nerve parathesia that may last for a year or more. A parathesia is defined as an altered sensation in the area served by the nerve. This may be numbness, tingling, burning or a crawling sensation. Rarely, are these sensations permanent, but when ever a nerve is manipulated the resulting trauma will have some affect on sensation.
A nerve called the inferior alveolar nerve runs through the lower jaw (mandible). This nerve gives sensory feeling to the lower lip and chin.
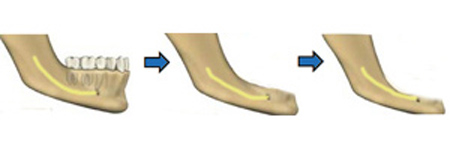
The inferior alveolar nerve (shown in yellow) lies below the teeth within the bone. After the teeth are lost the bone resorbs and the nerve becomes closer to the crest (top) of bone. When severe resorption has occurred, the inferior alveolar nerve may lie on top of the crest. After resorption starts there is less bone in the posterior mandible into which an implant can be placed without contacting the nerve.

In a cross section of the mandible we can see the relationship of the inferior alveolar nerve with regard to the tooth when it is present. Following extraction of the tooth we can see that as bone resorption occurs the nerve gets closer to the crest. This can make implant placement a challenge as there is less available bone to accommodate the nerve without interference with the nerve.
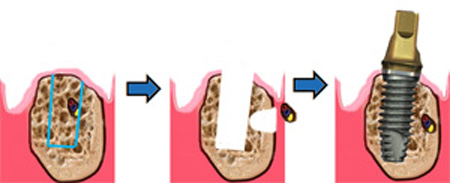
A technique was developed in the 1970’s by Dr. Hilt Tatum, where in the inferior alveolar nerve is moved out of its position to allow implant placement. As we can see in the illustration, the inferior alveolar nerve lies in the resorbed mandible where the implant needs to be positioned.
A channel is created and the nerve is moved out of the mandible allowing the site to be prepared for the implant. Following placement of the implant the nerves is placed in a new position and after healing the implants can be restored.
This technique is reserved for those patients who require implant placement in the posterior mandible and other methods are not suitable to allow the patient to be treated. Patients should be aware that there will be some parathesia (numbness) associated with the manipulation of the nerve but usually this is transient (temporary) and resolves in most patients after several months. The inferior alveolar nerve repositioning is typically a treatment performed by an oral surgeon and prior to accepting treatment for this procedure the process and possible complications are addressed.
Implant Cosmetic Dental Center™
----------------------------------------------------------------------------------------
Dr. Gregori M. Kurtzman is an international lecturer, selected as one of the top 100 dental speakers since 2006 by Dentistry Today, author of over 200 professional articles, a consultant to multiple dental manufacturers for product evaluation, development and research, he provides general dental care in suburban Maryland since 1986.
|
|
|
|
|
|
|
|
|
