|
|
|
|
|
| |
Quality general dental care with an emphasis on natural esthetics, form and function. Experience with complex restorative, prosthetic and implant treatment.
----------------------------------------------------------------------------------------
RESTORING TEETH:
Crowns, Onlays and Inlays
The mouth is divided into an upper and lower arch and each arch is then divided into an anterior segment and a posterior segment.
Anterior teeth are identified as the canines (cuspids), lateral incisors and central incisors. These are the teeth that are most prominent when we smile. The anterior teeth are designed to tear food, so that the back teeth can grind it and allow it to be digested.
Posterior teeth are identified as the molars and premolars (bicuspids) and a majority of our chewing are done on these teeth. The first molar, also know as the six year molar as it is the first permanent tooth to erupt at age six is often the first tooth filled.
Over a patients lifetime the filling may be replaced due to recurrent decay or fracture of the filling or tooth. Each time the old filling is removed and any decay with it the restoration becomes larger with less remaining tooth structure to retain the new restoration. When there is insufficient tooth structure to retain a new filling other treatments may become necessary to allow proper function of the tooth. There are various treatments that are dependent on how much tooth structure remains, including; bonded fillings, inlays, onlays and crowns.
During function the cusps of the teeth flex. When a filling is placed in a tooth the cusps are undercut in the case of amalgam (silver filling) and the cusps are weakened which may result in a fracture of the remaining tooth. This can also occur when bonded filling are placed but is less likely as they are chemically bonded. As the restoration becomes larger the likelihood of cuspal fracture increases dramatically. To allow normal function the amount of remaining tooth plays an important part in which restoration is best suited for the particular situation.
Bonded fillings also known as composites or white fillings are tooth colored restorations that are chemically bonded to the dentin and enamel of the tooth. They limit the degree of cuspal flexure close to a non-restored tooth. These are suited as a restortative choice when there is less than 40% of the tooth being replaced by the restoration. These are as strong or can be stronger than silver filling material. When more tooth is missing then other treatment choices are indicated. More information on tooth colored (bonded) fillings can be found at Tooth colored fillings.
Inlays, are laboratory fabricated restorations that are 3 to 5 times stronger than a bonded filling. These are utilized to replace missing tooth structure that lies within the cusps but requires more strength than a bonded filling can provide. Inlays can be fabricated from tooth colored materials such as porcelain or from cast gold. In high stress areas such as in molars of patients who clench or grind, cast gold is indicated over porcelain as it is fracture resistant and is much stronger material.
An Onlay is utilized when 70% or less of the tooth is being replaced by the restoration, when a cusp is missing or to protect the cusps from further damage. Onlays also know as 3/4 crowns, overlap the cusps and help strengthen the tooth and prevent cuspal flexure. These restorations also can be fabricated from tooth colored materials such as porcelain or cast gold. In molars due to the higher stresses and biting forces cast gold may be the material of choice due to its high strength. Tooth colored material serves well on premolars that require onlays as these teeth do not have the biting forces that occur on the molars.
When most of the tooth structure is missing or multiple cusps are being replaced a full coverage restoration known as a Crown (also referred to as a Cap ) is indicated. If the clearance is limited then a full cast gold crown can be placed or when sufficient space is present a porcelain fused to metal crown (PFM) can be utilized. A PFM crown consists of a metal coping onto which a tooth colored material is placed to increase the esthetics of the restoration. On premolars or in low stress situations on molars an all ceramic can be placed for maximum cosmetic results.
TYPES OF CROWNS
Crowns can be fabricated from several different materials; cast gold, porcelain fused to metal (PFM), porcelain to sintered gold, ceramic or compomer.
CAST CROWNS may be utilized in the posterior. If the tooth to receive the crown is short, it may be desired to place a cast gold crown as less tooth structure needs to be removed to secure the crown. This type of crown is made in a manner similar to jewelary, using the lost wax technique. These crowns are very strong but lack the esthetics of a natural looking tooth due to the color of the metal. These may be ideal for the molars where higher biting forces are generated on the teeth and are not visible.
Porcelain fused to metal crowns, also known as PFM crowns. These consist of a metal coping that is overlayed with porcelain to increase esthetics. These do require greater reduction of the tooth and may not be indicated for short molars. Due to the metal coping these do not look as esthetic as natural teeth due to increased opacity.
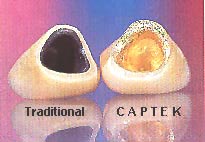
Porcelain to sintered gold crowns were introduced about about 20 years ago. Due to the high yellow color of the metal coping these provide a very esthetic result and can be used for single crowns anywhere in the mouth and for 3 unit bridges in limited situations. The original version consisted of a this gold sheet that was adapted to the die, trimmed then porcelain was fused over the gold. Currently, the technology has improved and the new technique either electo-plates 24k gold to the die or the material is adapted to a special die and baked to fuse it. Captek is an example of the "baked" technique.

Cermaic corwns are made entirely of ceramic with no metal underlaying structure. These can be made from several different processes; pressed, milled or layered.
Pressed ceramic crowns are made by using the lost wax technique and injecting molten ceramic to form a coping that porcelain is fused over to achieve the final result. Examples of pressed ceramic crowns are, Empress and cerapress. The ceramic used in pressed ceramics contains leucite. This acts to reinforce the ceramic and prevents micro cracks from spreading within the material. In feldspartic porcelain (the porcelain used for many years in dentistry) when a micro crack starts it spreads through the material until the ceramic fails due to severe fracture. When a micro crack starts within leucite containing porcelain, the crack propagates until it hits a leucite crystal and stops. Thermocycling studies have also found that these micro cracks self heal within leucite reinforced porcelains and may show better long term survival then feldspathic porcelain restorations.

Milled ceramic crowns are fabricated by scanning the die with a stylus, then a milling machine fabricates the ceramic coping from aluminum oxide. Porcelain is then fused over the coping. PROCERA is currently the only crown of this type on the market at this time. The coping is made of extremely dense-sintered aluminum oxide. The translucent coping offers remarkable esthetic characteristics, recreating the beauty of natural teeth.

Stylus scanning the die for the crown to be prepared.

Cut-a-way of a Procera crown showing the layering similar to natural tooth.
Examples of crowns:
CASE 1: Maxillary central incisors

Before

After
(placement of Cercon crowns on Maxillary central incisors)
CASE 2: Maxillary canine (cuspid)

Before

After
(placement of Cercon all ceramic crown on Maxillary canine)
Case 3: Maxillary lateral incisor

Before

After
(Replacement of an old worn acrylic and metal crown with a Porcelain fused to metal crown)
Case 4: Maxillary central incisor

Before

After
(Poorly shaded Porcelain fused to metal crowns has been replaced with an all ceramic crown that matches the shade of the adjacent teeth)
Implant Cosmetic Dental Center™
----------------------------------------------------------------------------------------
Dr. Gregori M. Kurtzman is an international lecturer, selected as one of the top 100 dental speakers since 2006 by Dentistry Today, author of over 200 professional articles, a consultant to multiple dental manufacturers for product evaluation, development and research, he provides general dental care in suburban Maryland since 1986.
|
|
|
|
|
|
|
|
|
